Tinnitus is a spontaneous, internally generated noise (often referred to as “ringing in ear”) which is heard in one or both ears. It is most often a subjective complaint, and the severity is dependent primarily on the patient’s description. It may occur alone or in combination with other symptoms such as: Temporo-Mandibular Joint (TMJ or TMD) issues, head, neck and back pain, dizziness (vertigo), and others.
Causes of Tinnitus
If there is no damage to the auditory system, and the tinnitus is subjective (heard by individual only), it is likely caused by one of these:
- Jaw Joint Dysfunction (TMJ or TMD)
- Chronic neck muscle strain (most often related to TMD)
- Trauma (most often related to TMD)
- Occlusal changes (most often related to TMD)
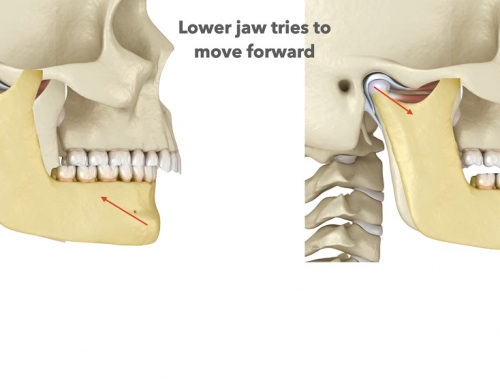
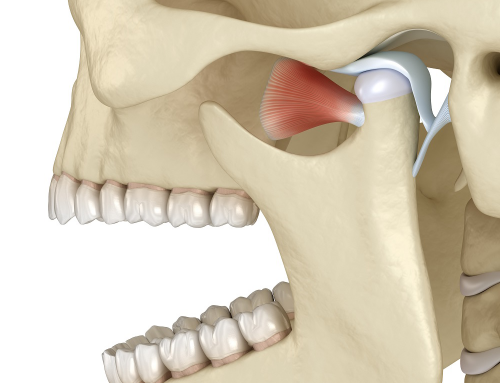
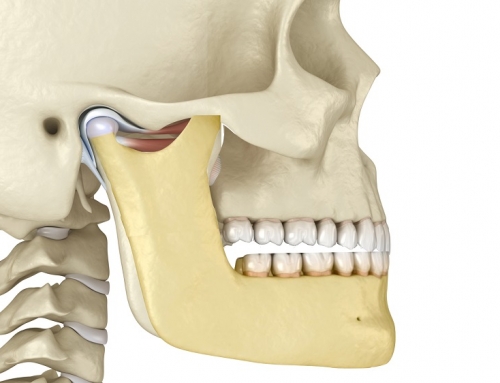
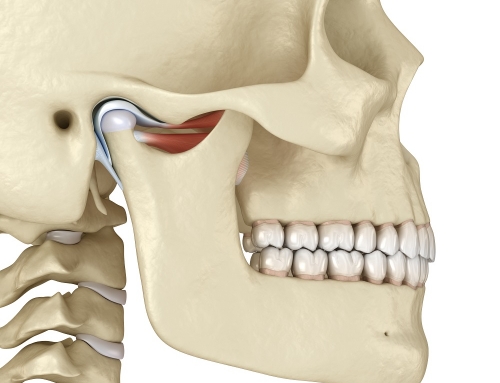
There have been many attempts to explain the association between TMJ and tinnitus in the dental literature. One speculation is that pressure from the condyle could cause eustachian tube blockage, causing tinnitus. Another hypothesis was based on the common nerve supply to the masticatory muscles and tensor veli palatini muscle, and speculated that hyperactivity of the masticatory muscles could induce a secondary reflex contraction of the tensor veli palatini muscle, congestion of the middle ear, and consequently tinnitus. Others have proposed the concept that the middle and inner ears receive input from the Trigeminal Nerve and Sympathetic nerves of the middle ear through the tympanic plexus and this may be responsible for tinnitus. Other research points to the masseter muscle trigger points as well as inflammation within the TMJ.
Treatment of Tinnitus
Treatment can be frustrating for the treating physician who often prescribes tranquilizers and muscle relaxants in an effort to control muscle contraction. Currently, doctors believe that the majority of cases of tinnitus arise from anomalies in one or more of the elements of the neural chain that makes up the auditory nervous system. In the recent years, expert dentists treating patients from the neuromuscular approach have had success in alleviating tinnitus. It is recommended that an ENT carries out a neurological evaluation prior to initiating neuromuscular treatment.
It has been reported that TMD therapy improves tinnitus in up to 96% of patients who have TMD and co-existing tinnitus. The neuromuscular dentist has the ability to measure masticatory muscle activity at rest and in function and, by restoring the masticatory and associated muscle activity to optimal function and rest, TMD complaints of tinnitus usually resolve.