 Examination and palpation of the muscles involved directly and indirectly in mouth opening and closing is key to a thorough TMJ exam. Since much of the pain caused by TMD is muscle-related, it becomes very important for the clinician to learn which muscles are affected in a TMD patient.
Examination and palpation of the muscles involved directly and indirectly in mouth opening and closing is key to a thorough TMJ exam. Since much of the pain caused by TMD is muscle-related, it becomes very important for the clinician to learn which muscles are affected in a TMD patient.
Primary Muscles
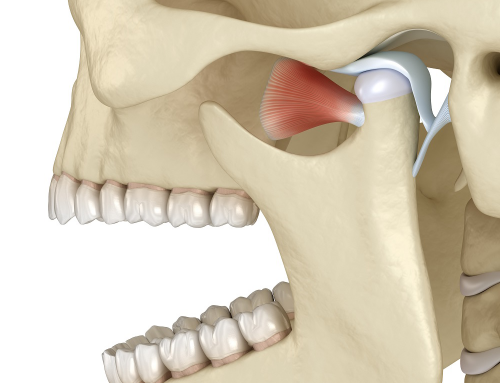
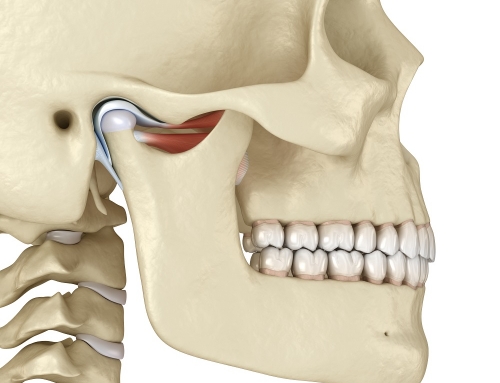
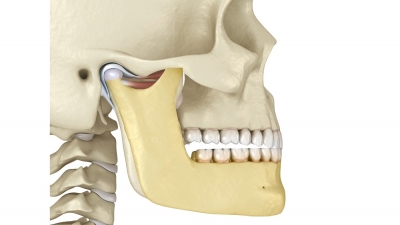
The primary muscles directly involved in mandibular closure are the Masseter and the Temporalis. The Medial Pterygoid muscle is responsible for closing and lateral movements of the mandible. The lateral Pterygoid muscle is responsible for opening, deviation to either side, and anterior movement of the mandible.
Secondary Muscles
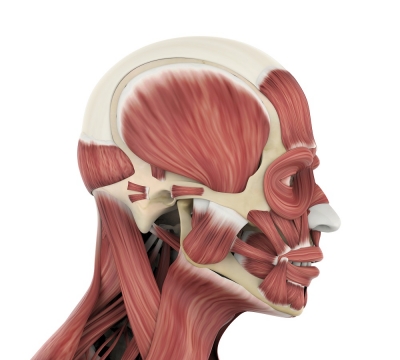
The secondary muscles directly involved with mandibular function are sets of paired muscles, which coordinate the full integration of mandibular movement during opening and closing through their attachments to the hyoid bone, the mandible, and other bones. These are the: digastric, geniohyoid, mylohyoid, omohyoid, sternohyoid, sternothyroid, stylohyoid, and thyrohyoid.
The secondary muscles indirectly associated with mandibular function are in the cervical area and attach to the sternum, temporal bone, clavicle, cervical vertebrae 1-7, and ribs 1-2. These muscles stabilize the skull and neck and allow the mandible to move relative to the skull.
Other muscles indirectly associated with mandible position are as follows:
Sternocleidomastoid – the role of this muscle is to rotate the head to the opposite side, balancing the head especially if the mandible is higher on one side vs the other.
Trapezius – this muscle plays an important role in posture. If one side of the head and neck are rotated or tilted, the traps will step in to maintain balance on the opposing side, causing pain or muscle tension as a result.
Buccinator – this muscle compresses the cheeks inwards against the molars, helping in chewing and swallowing. If the vertical height of the mandible related to the maxilla is reduced, the buccinator will often play a role in stabilizing the occlusal plane by creating a cushion between the posterior teeth and result in scalloping.
Head Position & Posture
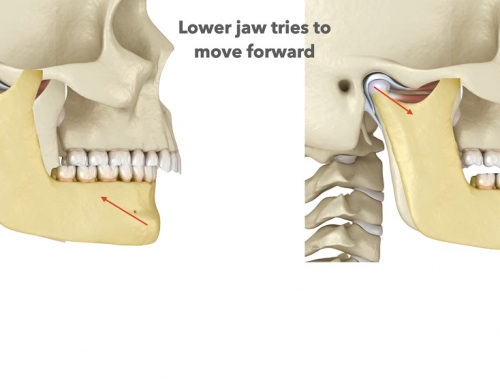
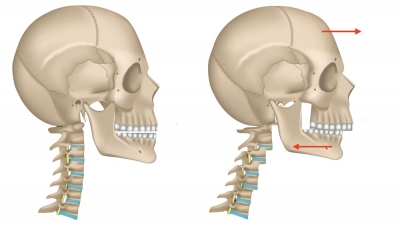
The majority of TMD-related muscle pain is due to muscle tension. In cases where the mandible retrudes in order for posterior teeth to touch (found frequently in class 2 cases, and in vertical over-closure), the head must come forward in order to balance. As the body tries to readjust in order to maintain that balance, the person begins to bring their head forward, tilting at the atlas (C1), engaging the axis (C2), and involving C3-C7 vertebrae so that they can hold that position. Many TMD patients have a forward-head position when standing and, if one side of the mandible is affected more than the other, you will also see the shoulder level asymmetry as a result, balancing in all 3 dimensions.
Muscles & Balance
In order to manage all these postural changes due to the retruded mandible, the muscles have to constantly flex or contract to hold that mandible in place during chewing and swallowing. When a person swallows, their posterior teeth come together into contact, and that occurs approximately 2000 times a day. So the masseter has to contact to bring the mandible up, the medial pterygoid has to contract to help in this elevation, the temporalis has to contract to bring the mandible back, and the posterior neck and shoulder muscles all step in to coordinate this constant flexing.
Now what happens if a muscle is in constant and chronic contraction? The muscle fibres are shorter when flexed and that creates tension. Constant chronic tension is what causes muscles to spasm and creates pain. Many of these patients suffer in debilitating pain in the head, neck and shoulder area, but nothing will show up on routine medical exams. ENT specialists will find nothing wrong with the patient, scans for tumours will yield no results, and the patient goes back to their doctor, only to receive a prescription for pain medication or anti-depressants. Alternative therapy like acupuncture, chiropractic, massage, may provide temporary relief, but as the mandible continues to retract, engaging the same muscles over and over, pain returns and the patient continues to suffer.