Imaging
In all cases of suspected TMD, imaging will be required to support a diagnosis and eliminate possible other conditions. One of the most basic and initial radiographs used is the panorex. One of the important things to recognize is that the panorex actually does not tell us much about the jaw joint. It does show the jaw and the associated structures and is a helpful tool in identifying any periodontal or odontogenic causes for orofacial pain. A panoramic x-ray essentially rules out other possible causes of pain in the TMJ region, and allows the clinician to begin assessment by narrowing down the possible causes. A panorex does allow the clinician to assess bony changes in the masseter insert region as well as stylohyoid ligament calcifications, which are both signs of chronic excessive clenching and grinding, and extremely common in TMD patients with symptoms.
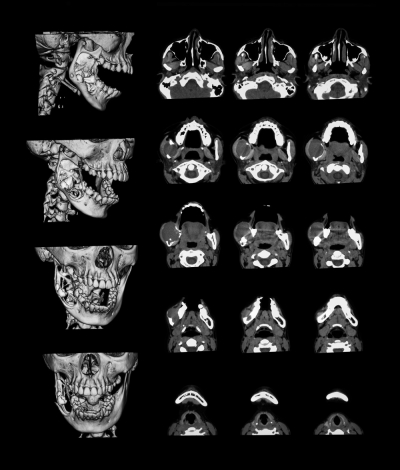
In patients with symptoms, once other possible causes are ruled out by the panorex, additional imagining is usually required in order to finalize the diagnosis. This includes a CBCT, MRI or other imaging to visualize the condyle, disc position, and degeneration of the jaw joint.
Possible Diagnosis
Assessment of TMD patients with dysfunction usually leads to one of the following diagnoses:
- Disc Displacement with reduction – reproducible click on opening and closing
- Disc Displacement without reduction – history of joint noise and limitation of mandibular opening but no click present currently. Slight limitation of opening. Limitation o the affected side or both
- Capsulitis – tenderness of TMJ with range of motion limited by pain; no crepitus
- Osteoarthritis – tenderness of TMJ (laterally or in ear canal on palpation) with crepitus
- Rheumatoid arthritis – same as Osteoarthritis but pt confirms medical diagnosis of RA
- There are other possible diagnoses and a definitive statement cannot be made until further testing is completed and confirmed.